

Increasing use of ORS and zinc to treat child diarrhea in Uganda
|

In low-resource countries, diarrhea is one of the leading causes of death among children under age five. Oral rehydration solution (ORS) is a simple, low-cost, and highly effective treatment for diarrhea. Unfortunately, fewer than half of children with diarrhea receive ORS. Even fewer receive both ORS and zinc, which is the World Health Organization’s recommended treatment.
To help inform efforts to increase ORS and zinc access, we conducted a study in Uganda in 2017 using community health worker (CHW) programs. Like many countries, Uganda uses CHWs to increase access to essential health products such as ORS and zinc. Some CHW programs charge for health products, whereas others distribute products for free. Additionally, some CHWs deliver products to homes, while others others require that caretakers retrieve products from a central location. Because there is little evidence about which variations increase usage of ORS, we designed a study to evaluate price and inconvenience as barriers to ORS use.
We worked with CHWs from the nonprofit organization BRAC to conduct tests, randomizing 188 villages (and their CHWs) into 4 groups. The first group delivered free ORS and zinc to all households before any child was ill. In this arm, free ORS and zinc were already conveniently available inside the home when a child came down with diarrhea. In the second group, CHWs informed caretakers in advance that ORS and zinc were both available for free from the CHW’s home in case their child came down with diarrhea. This arm provided ORS for free, but without the convenience of home delivery. In the third group, CHWs visited all households and offered to sell ORS and zinc in advance of illness at the market price. This arm offered convenience, but with a cost. The fourth group served as a control by having CHWs carry out their normal activities.
To carry out the study, we offered a training session for all CHWs in the first three groups and provided each CHW with sufficient free ORS to serve all of the children under five years of age in their village.
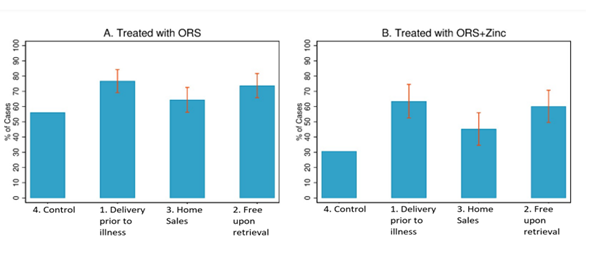
The interventions substantially increased ORS use. Only 56% of control group cases received ORS. In contrast, 76% of cases in Group 1 (free home delivery prior to illness) and 74% of cases in Group 2 (free upon retrieval by the caretaker) received ORS. Group 3 (home sales prior to illness) treated 64% of cases. And while only 30% of control group cases received both ORS and zinc, that percentage increased to 62%, 58%, and 46% in Groups 1, 2, and 3, respectively.
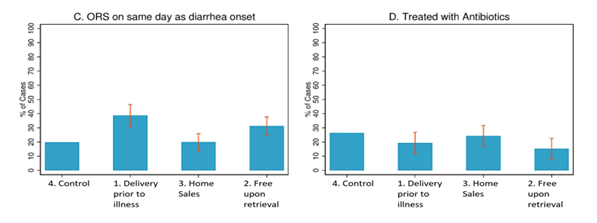
The likelihood of starting ORS on the first day of symptoms also increased with free home delivery and free retrieval by caretaker. Additionally, undesirable use of antibiotics for uncomplicated diarrhea cases—which can contribute to drug resistance—was slightly lower in the free retrieval group.
Interestingly, we found that CHWs were more motivated to distribute ORS and zinc for free than when charging the market price, even though CHWs kept all revenue with home sales. For example, CHWs in the free retrieval group visited nearly 70% more households than CHWs in the home sales arm. These findings suggest that many CHWs may respond more to the opportunity to help their neighbors than to the opportunity to earn a modest amount of money.
Our results showed that implementing either free distribution or retrieval by caretaker increases ORS use. If implemented nationwide in Uganda, these approaches could avert over 1200 child deaths per year.
ORS and zinc are among the most cost-effective child health interventions available. Simple changes in distribution methods could help ensure that all children benefit.
Contact the authors:
Wagner: zwagner@rand.org
Asiimwe: asiimweajb@gmail.com
Dow and Levine: levine@berkeley.edu






