The biggest scandal in global health today: Why are 2 million children dying from pneumonia and diarrhea every year?
|

On a recent visit to a local children's ward in the northern part of Ethiopia over 70% of the children were suffering from pneumonia. When a child in this region goes to the hospital, most often the parents move in as well, sleeping in the same bed and living there until they are discharged.
Global health is like a juggernaut. It is very hard to turn around if it gets set on the wrong course. Yet when it comes to the health of the world's most vulnerable children, this is basically what has to be done if we want to save children's lives on the scale required to achieve global health goals. We need to turn the juggernaut around and set it on a path towards a new goal - fighting the leading killers of children.
If you don't work in global health you might be surprised to learn that fighting the leading killers of children has not been a global priority. You might also be surprised to learn exactly what the leading killers of children under 5 are - two diseases, pneumonia and diarrhea. These two kill more children under 5 than AIDS, malaria and measles combined. They cause 2 million children to die every year and account for a massive 30% of all under 5 deaths. And yet they attract less than 5% of global health funding.
To add insult to injury we have very cost effective vaccines, antibiotics and other treatments like oral rehydration salts and zinc that can prevent and treat the leading causes of pneumonia and diarrhea. If we made them widely available, pneumonia and diarrhea would kill a fraction of the children that they do now. Vaccines alone have the power to prevent almost 1 million child deaths from pneumonia and diarrhea every year. When you add in antibiotics, oral rehydration salts, zinc and vitamin A supplements - each of which cost cents per dose - you can probably double that figure and wipe out almost all deaths.
So why haven't we done it? The answer has a lot to do with our global health architecture and our failure to mobilize and focus global health resources on the areas where the greatest number of children can be saved - and of course the two are related. We have separate organizations that deliver vaccines, medicines and nutritional supplements and they typically compete over scarce donor dollars rather than collaborate to introduce these interventions in the countries where most children are dying. They are rewarded for the amount of funding they can attract rather than for the number of children's lives they are actually saving, so the incentive is to focus their resources on raising money rather than collaborating to save children.
If we did have one global health organization responsible for halving child mortality by 2015 - saving about 3.5 million lives per year - with the power and resources to coordinate vaccine delivery with access to antibiotics and other interventions, you would start to see some real progress. And if that organization focused on the most vulnerable children in the countries where child deaths are concentrated - India, Nigeria, Democratic Republic of Congo, Pakistan, Ethiopia, Afghanistan and China (precisely the countries where our existing health organizations often struggle to have impact), then you would start to see child mortality reductions on the scale required to achieve global health goals.
But we don't live in a perfect world and we won't see a more effective global health architecture anytime soon. So what can we do in the countdown to 2015 to save more children from pneumonia and diarrhea? We can continue to argue that the big donors in child health put pneumonia and diarrhea to the top of their lists. We can ask the major UN agencies and NGOs in child health to account for the proportion of their budgets allocated to pneumonia and diarrhea - are they spending ~30% to fight the leading killers of children? We can create structures that make it easier for all partners to collaborate in the regions where child deaths are concentrated because if we want to achieve impact at scale, we have to work at scale and that is beyond the capacity of any one organization.
We need large, multi-stakeholder public-private partnerships mobilized against pneumonia in the northern states of India and the northern states of Nigeria and we need the prevention and treatment communities working hand in glove to reach the most vulnerable children in these critical geographic areas. And we need World Pneumonia Day! Because the real value of this day is to shine a light on all of these opportunities and to draw together the many stakeholders committed to advancing the health of children so we can save more children, quickly.
-- Leith Greenslade is Co-Chair of Child Health at the MDG Health Alliance. The Alliance operates in support of Every Woman Every Child, an unprecedented global movement spearheaded by the United Nations Secretary-General to mobilize and intensify global action to improve the health of women and children. We work closely with many partners, especially the UN Foundation, the Partnership for Maternal, Newborn and Child Health, and the Global Compact to help optimize the engagement of the private sector toward the goals of Every Woman Every Child.The Alliance is comprised of eminent leaders from the private, public, and nonprofit sectors working in conjunction with the Health and Education Cluster of the Secretary General's MDG Advocates.
For more information:
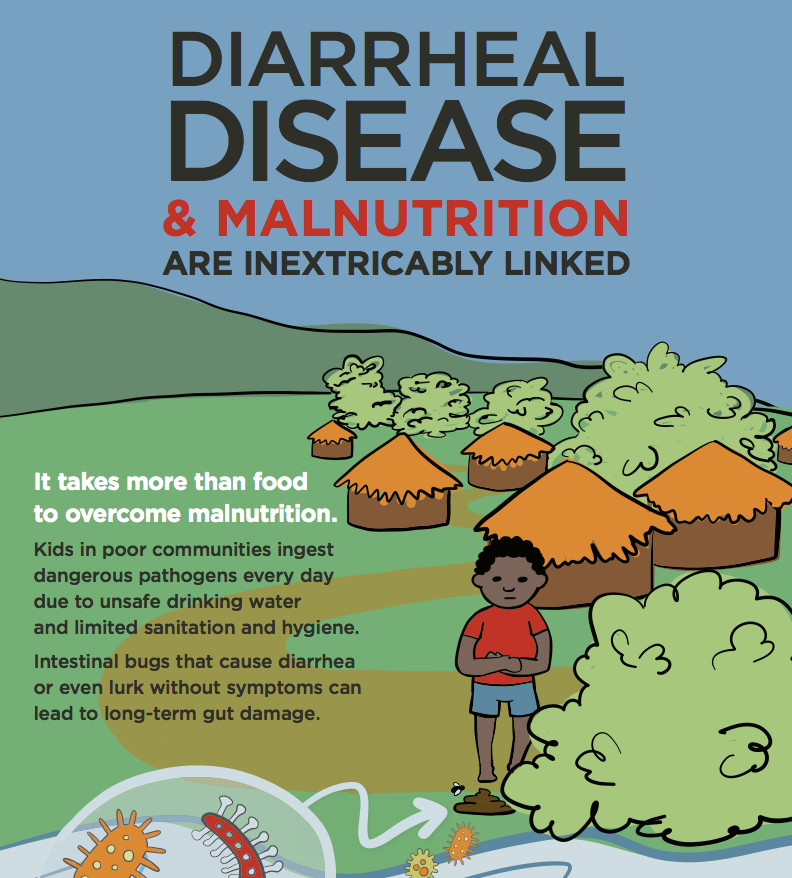
-- INFOGRAPHIC: Tackling the deadliest diseases for the world's poorest children.
Photo credit: David Rotbard